Introduction
All herpes viruses can develop a latent state within specific tissues, in which they rest until reactivation. Reactivation is triggered by menstruation, anxiety states, fever, sunlight exposure, or weakening of the immune system. Viruses cause cells to become multinucleated giant syncytial cells with intranuclear inclusion bodies, and cause local destruction when they migrate to the peripheral skin. Disease is resisted by cell-mediated immunity, but the virus remains latent in nerve cells throughout one's life.
Only alpha subfamily viruses (herpes simplex 1 and 2, and varicella zoster) cause cell damage to the skin.
Herpes simplex virus 1 & 2
Latent in nerve cell bodies. HSV-1 produces most cold sores and HSV-2 produces most genital herpes. Symptoms include watery blisters in the skin or mucous membranes of the mouth, lips or genitals. Herpes simplex can be spread through contact with saliva. HSV infection during pregnancy can result in transplacental viral transfer (by crossing the blood-placenta barrier).
Varicella zoster virus
Latent in nerve cell bodies. Causes varicella (chickenpox) AND herpes zoster (shingles). A breakout of shingles causes painful skin rashes.
Cytomegalovirus
Latent in salivary glands, and dendritic and myeloid cells. CMV infects both epithelial cells and various cells of the immune system. Infection is typically unnoticed in healthy people, but can be life-threatening for the immunocompromised. CMV causes four infectious states: (1) Asymptomatic (2) Congenital disease in infants by transmission from mother, causing mental retardation (3) Mononucleosis syndrome in young adults (4) Reactivation, causing retinitis (blindness), pneumonia or disseminated infection.
Epstein-Barr virus
Latent as multiple copies of circular DNA. Causes mononucleosis by infecting B cells, and is involved in certain cancers. EBV causes cells to "transform" and act as cancer cells, passing on copies of EBV DNA to their progeny. However, malignant cells are cleared by the immune system, with the resolution of mononucleosis illness.
Tuesday, June 10, 2014
Monday, June 9, 2014
Hepatitus Viruses
Introduction
There are five main hepatitis viruses (types A, B, C, D and E) that infect the liver. F and G are not considered to be dangerous. Only hepatitis B (and hepatitis F) viruses are DNA viruses; the remaining types are RNA viruses. All hepatitis viruses are parenteral transmission except for A and E, which are fecal-oral transmission.
Symptoms
Acute (lasting fewer than 6 months)
Initial non-specific flu-like symptoms. May include fatigue, fever, headache, muscle and joint aches, coughing, vomiting, and diarrhea. Many hepatocyte death results in the release of high levels of cell enzymes AST and ALT. Some pericanalicular (bile duct lining) cell death results in low levels of GGT and alkaline phosphatase. The presence of these enzymes in the blood is a sign of hepatitis.
As the liver swells, the bile duct becomes blocked, causing a backup of bilirubin to the blood. In 1-2 weeks, the buildup of bilirubin leads to jaundice due to the liver's failure to metabolize and excrete bilirubin.
Chronic
Often asymptomatic, with enlarged liver and mildly elevated liver enzyme levels in the blood. A first-time, acute hepatitis infection can become chronic if the virus is not cleared in 6 months.
HAV
Frequently affects young children. Transmitted by fecal-oral route from poor hand washing, or from ingesting contaminated water.
HBV
Virus lives in all fluids of an infected patient. Transmitted by blood and sexual contact. Only 10% develop chronic hepatitis.
HCV
Leading cause of chronic hepatitis in the United States. 85% develop chronic hepatitis from acute infections. Transmitted parenterally primarily via injections from drug use.
HDV
Replicates only with the help of HBV by using the envelope of HBV to cause infection. An HDV infection to a chronic HBV carrier results in severe acute hepatitis. As carriers can't make antibodies against HBV, they also become carriers of HDV.
HEV
Similar to HAV. Endemic to Asia, India, Africa, and Central America.
There are five main hepatitis viruses (types A, B, C, D and E) that infect the liver. F and G are not considered to be dangerous. Only hepatitis B (and hepatitis F) viruses are DNA viruses; the remaining types are RNA viruses. All hepatitis viruses are parenteral transmission except for A and E, which are fecal-oral transmission.
Symptoms
Acute (lasting fewer than 6 months)
Initial non-specific flu-like symptoms. May include fatigue, fever, headache, muscle and joint aches, coughing, vomiting, and diarrhea. Many hepatocyte death results in the release of high levels of cell enzymes AST and ALT. Some pericanalicular (bile duct lining) cell death results in low levels of GGT and alkaline phosphatase. The presence of these enzymes in the blood is a sign of hepatitis.
As the liver swells, the bile duct becomes blocked, causing a backup of bilirubin to the blood. In 1-2 weeks, the buildup of bilirubin leads to jaundice due to the liver's failure to metabolize and excrete bilirubin.
Chronic
Often asymptomatic, with enlarged liver and mildly elevated liver enzyme levels in the blood. A first-time, acute hepatitis infection can become chronic if the virus is not cleared in 6 months.
HAV
Frequently affects young children. Transmitted by fecal-oral route from poor hand washing, or from ingesting contaminated water.
HBV
Virus lives in all fluids of an infected patient. Transmitted by blood and sexual contact. Only 10% develop chronic hepatitis.
HCV
Leading cause of chronic hepatitis in the United States. 85% develop chronic hepatitis from acute infections. Transmitted parenterally primarily via injections from drug use.
HDV
Replicates only with the help of HBV by using the envelope of HBV to cause infection. An HDV infection to a chronic HBV carrier results in severe acute hepatitis. As carriers can't make antibodies against HBV, they also become carriers of HDV.
HEV
Similar to HAV. Endemic to Asia, India, Africa, and Central America.
Thursday, June 5, 2014
Influenza Viruses (Orthomyxoviridae and Paramyxoviridae)
 Structure
StructureViruses are spherical, containing negative stranded RNA; outer membrane contains hemagglutinin activity (HA) and neuraminidase activity (NA) glycoproteins that are anchored to the inner lipid bilayer by M-proteins.
Hemagglutinin
Attachment to host cell sialic acid receptors, which are found on the surface of red blood cells, and upper respiratory tract cells. HA is needed for absorption of the viral genome.
Neuraminidase
Cleaves neuraminic acid of the mucin upper respiratory barrier to expose sialic acid receptors; also cleaves sialic acid receptor to avoid attachment of budding viruses, which will escape to infect new cells.
In paramyxoviruses, HA and NA are part of the same glycoprotein spike. They also contain fusion protein (not found in orthomyxoviruses) that causes the infected cells to fuse into giant multinucleated cells.
Orthomyxoviridae
Orthomyxoviruses are influenza viruses, of which there are three types. Type A infects humans, other mammals, and birds, whereas type B and C infect only humans. Type A causes the most severe disease, with Type B and C in decreasing severity.
Paramyxoviridae (colds/flu in adults, pneumonia in children, measles, mumps)
Paramyxoviruses include parainfluenza viruses, respiratory syncytial virus (RSV), metapneumovirus, mumps virus, and measles virus.
Metapneumovirus causes upper and lower respiratory tract infections primarily in young children or elderly. Parainfluenza and RSV cause upper respiratory infections that have cold-like symptoms in adults, but produce influenza-like sickness from lower respiratory tract infections (bronchiolitis, viral pneumonia, croup) in children, elderly, and immunocompromised patients.
Sunday, March 23, 2014
Amino Acids
Functions
Amino acids have interconnections with other biochemical processes of the body. They can be used for energy (ketogenic), or be converted to glucose (glucogenic). Ketogenic amino acids can convert directly to acetyl CoA, while glucogenic amico acids can convert to intermediate molecules in the Krebs cycle, which can contribute to the synthesis of glucose.
Amino acids also contribute to the formation of nucleic acids, spingolipids, hormones, peptides, and other molecules.
Mnemonics
Essential 10
"Private Tim Hall" (Phe Val Thr Trp Ile Met His Arg Leu Lys).
Purely ketogenic
Only leucine and lysine are not glucogenic.
Both glucogenic and ketogenic
"Tip" ([Thr Tyr Trp] Ile Phe).
The remaining amino acids are purely glucogenic.
Excretion
Excess amino acids are not stored, so they are used as energy or converted into other molecules. In this conversion, the -NH2 groups are removed (by transamination), transported, and excreted as urea:
Amino acids have interconnections with other biochemical processes of the body. They can be used for energy (ketogenic), or be converted to glucose (glucogenic). Ketogenic amino acids can convert directly to acetyl CoA, while glucogenic amico acids can convert to intermediate molecules in the Krebs cycle, which can contribute to the synthesis of glucose.
Amino acids also contribute to the formation of nucleic acids, spingolipids, hormones, peptides, and other molecules.
Mnemonics
Essential 10
"Private Tim Hall" (Phe Val Thr Trp Ile Met His Arg Leu Lys).
Purely ketogenic
Only leucine and lysine are not glucogenic.
Both glucogenic and ketogenic
"Tip" ([Thr Tyr Trp] Ile Phe).
The remaining amino acids are purely glucogenic.
Excretion
Excess amino acids are not stored, so they are used as energy or converted into other molecules. In this conversion, the -NH2 groups are removed (by transamination), transported, and excreted as urea:
- By transamination, 2-ketoglutarate transfers its oxygen to the amino acid while removing and taking on the -NH2 group to form glutamate. (2-ketoglutarate is a Kreb's cycle intermediate, and a nitrogen transporter).
- Glutamate travels to the liver and releases ammonia (oxidative deamination) to the urea cycle. In the process, glutamate changes back to 2-ketoglutarate.
Saturday, March 22, 2014
Lipids
Fatty acid synthesis and oxidation
The synthesis and breakdown of fatty acid chains are due to repetitive cycles that add and remove two carbons each time. Synthesis occurs in the cytosol while oxidation occurs in the mitochondrion. In the breakdown cycle, energy molecules NADH, FADH2 and acetyl CoA are produced, which results in 17 ATPs for each two-carbon loss.
Hormonal controls
When blood sugar is low, epinephrine, norepinephrine and glucagon stimulate lipase in fat cells to break down triglycerides. The glycerol can then be used to produce more glucose.
In contrast, insulin promotes the transport of glucose into cells, where glucose is converted and stored as triglyceride. Insulin also inhibits lipid breakdown through several mechanisms and increases synthesis of glycogen, fatty acids, triglycerides and proteins.
Ketones
In states of starvation, fatty acid breakdown results in the four-carbon acetoacetyl CoA. Acetoacetyl CoA can break down further to acetyl CoA, be used for synthesis of cholesterol, or change to ketones. Ketones may be used for fuel by the brain as a last resort.
Lipids
Fatty acids are stored on the three-carbon glycerol, forming glycerides. Triglycerides are the main storage molecules, which can revert to fatty acids and glycerol - to be used for cellular energy (glycerol to glycerol 3-P to glyceraldehyde 3-P). Acetyl CoA from the energy pathways with glycerol can form triglycerides. Therefore, excess sugar from the diet goes into glycerol to fatty acids (via acetyl CoA) to triglycerides, which are stored in fat cells.
Phosphoglycerides
Glycerol can also form phosphoglycerides when attached to phosphate attached to serine, ethanolamine, choline or inositol. Compared to triglycerides, phosphoglycerides are esters of only two fatty acids, and are important membrane components.
Prostaglandins
Prostaglandins are fatty acids synthesized throughout the body, having hormone-like effects.
Sphingolipids
These molecules contain two fatty acids and a third group linked to the three-carbon serine. They are found in the nervous system.
Cholesterols
Cholesterol is ingested, but also synthesized from acetyl CoA, which transforms to isoprene. Isoprenes are the five-carbon building block forming isoprenoid molecules, or cholesterols. Cholesterol may then become bile acids and salts (mainly produced and exported by the liver), or form various steroid hormones.
The synthesis and breakdown of fatty acid chains are due to repetitive cycles that add and remove two carbons each time. Synthesis occurs in the cytosol while oxidation occurs in the mitochondrion. In the breakdown cycle, energy molecules NADH, FADH2 and acetyl CoA are produced, which results in 17 ATPs for each two-carbon loss.
Hormonal controls
When blood sugar is low, epinephrine, norepinephrine and glucagon stimulate lipase in fat cells to break down triglycerides. The glycerol can then be used to produce more glucose.
In contrast, insulin promotes the transport of glucose into cells, where glucose is converted and stored as triglyceride. Insulin also inhibits lipid breakdown through several mechanisms and increases synthesis of glycogen, fatty acids, triglycerides and proteins.
Ketones
In states of starvation, fatty acid breakdown results in the four-carbon acetoacetyl CoA. Acetoacetyl CoA can break down further to acetyl CoA, be used for synthesis of cholesterol, or change to ketones. Ketones may be used for fuel by the brain as a last resort.
Lipids
Fatty acids are stored on the three-carbon glycerol, forming glycerides. Triglycerides are the main storage molecules, which can revert to fatty acids and glycerol - to be used for cellular energy (glycerol to glycerol 3-P to glyceraldehyde 3-P). Acetyl CoA from the energy pathways with glycerol can form triglycerides. Therefore, excess sugar from the diet goes into glycerol to fatty acids (via acetyl CoA) to triglycerides, which are stored in fat cells.
Phosphoglycerides
Glycerol can also form phosphoglycerides when attached to phosphate attached to serine, ethanolamine, choline or inositol. Compared to triglycerides, phosphoglycerides are esters of only two fatty acids, and are important membrane components.
Prostaglandins
Prostaglandins are fatty acids synthesized throughout the body, having hormone-like effects.
Sphingolipids
These molecules contain two fatty acids and a third group linked to the three-carbon serine. They are found in the nervous system.
Cholesterols
Cholesterol is ingested, but also synthesized from acetyl CoA, which transforms to isoprene. Isoprenes are the five-carbon building block forming isoprenoid molecules, or cholesterols. Cholesterol may then become bile acids and salts (mainly produced and exported by the liver), or form various steroid hormones.
 |
| Steroidogenesis by David Richfield and Mikael Häggström |
Friday, March 21, 2014
Carbohydrates
An energy source
The pentose phosphate pathway, or the hexose monophosphate (HMP) shunt, is a way to produce energy in the form of NADPH from the oxidation of six carbon sugars. It is an alternative to glycolysis, but its primary role is anabolic rather than catabolic: the transformation of sugars with the release of CO2 produces the five carbon ribose, which can be used for DNA and RNA synthesis. Also, if there is a need for NADH, FAD or CoA, ribose can be converted to glyceraldehyde 3-phosphate used in glycolysis.
The PPP is found throughout the body, in fat and liver cells, which use NADPH for fatty acid synthesis and (in liver) for cholesterol synthesis. Red blood cells lacking mitochondria use this pathway as an important source of energy.
Carbohydrate storage / Glycogen breakdown
Steps of glycogen formation:
Enzymes of glycogen breakdown:
Note that glycogen can only be broken down to glucose or glucose 1-P. Unlike glucose, glucose 1-P does not easily cross membranes, so it is preferred by cells in the muscle or liver.
The pentose phosphate pathway, or the hexose monophosphate (HMP) shunt, is a way to produce energy in the form of NADPH from the oxidation of six carbon sugars. It is an alternative to glycolysis, but its primary role is anabolic rather than catabolic: the transformation of sugars with the release of CO2 produces the five carbon ribose, which can be used for DNA and RNA synthesis. Also, if there is a need for NADH, FAD or CoA, ribose can be converted to glyceraldehyde 3-phosphate used in glycolysis.
The PPP is found throughout the body, in fat and liver cells, which use NADPH for fatty acid synthesis and (in liver) for cholesterol synthesis. Red blood cells lacking mitochondria use this pathway as an important source of energy.
Carbohydrate storage / Glycogen breakdown
Steps of glycogen formation:
- Glucose
- Glucose 6-P
- Glucose 1-P
- UDP-glucose (addition of ribose sugar UTP)
- Amylose (unbranched)
- Glycogen (branched)
Enzymes of glycogen breakdown:
- Phosphorylase breaks apart glucose units, but cannot break 1-6 branching. Glucose units are phosphorylated to become glucose 1-P.
- Debranching enzyme breaks down branched residue, producing more glucose 1-P.
- Salivary and pancreatic amylase can break down starch directly to maltose, which can then split to glucose by maltase.
- Lysosomal alpha-glucosidase, found throughout the body, converts glycogen directly to glucose.
Note that glycogen can only be broken down to glucose or glucose 1-P. Unlike glucose, glucose 1-P does not easily cross membranes, so it is preferred by cells in the muscle or liver.
Thursday, March 20, 2014
Cellular Energy
Energy molecules
ATP is the body's main energy molecule. Energy is stored in forms of glycogen or triglyceride, which can be broken down to regenerate ATP. Some high-energy molecules include:
A note about enzymatic biochemistry reactions
Enzymes and substrates of a reverse reaction are usually found in a different area of the body, so forward and reverse reactions do not compete. If a two-way reaction is found in the same area, then negative (or positive) feedback of enzymes prevent a "futile cycle" (competition within two-way reactions).
ATP production
Glycolysis occurs in all organ cells, producing two pyruvates per glucose. Pyruvate is converted to acetyl CoA, which can enter the Krebs cycle. Besides glycolysis, acetyl CoA can also be formed through fatty acid degradation or by transformation of certain amino acids.
Glycolysis (cytosol)
Produces 2 pyruvate, net 2 ATP and 2 NADH per glucose.
Anaerobic glycolysis (cytosol)
The Krebs cycle needs O2 to run, otherwise anaerobic glycolysis will occur. It is like glycolysis with an extra step: cycle the 2 NADH to replenish 2 NAD+ via transformation of 2 pyruvate to 2 lactate. Net 2 ATP.
Pyruvate decarboxylation (mitochondria)
Produces 2 acetyl CoA and 2 NADH per glucose.
Krebs cycle and Oxidative phosphorylation (mitochondria)
Including pyruvate decarboxylation, the Krebs cycle produces 1 ATP, 1 GTP, 8 NADH, and 2 FADH2 per glucose. In the electron transport chain, phosphorylation (ATP production) is coupled with oxidation (requiring O2 at the end).
Based on newer sources, 2.5 ATP are generated per NADH in the mitochondria. 1.5 ATP are generated per NADH in the cytosol, and per FADH2. This is a total of 30-32 ATP per glucose in aerobic respiration.
Note that the presence of ADP stimulates oxidation, and the lack of ADP (and abundance of ATP) slows the rate of oxidation.
Connections to other processes
Glyceraldehyde 3-P (halves of glucose) can be directed back towards gluconeogenesis, or towards acetyl CoA and the Krebs cycle. Amino acids can be transformed into acetyl CoA or other molecules in the Krebs cycle, and vice versa. Acetyl CoA is also used to generate lipids (lipogenesis). Succinyl CoA can be used to produce heme molecules, while other molecules from the Krebs cycle can be used to make purines and pyrimidines for DNA synthesis.
ATP is the body's main energy molecule. Energy is stored in forms of glycogen or triglyceride, which can be broken down to regenerate ATP. Some high-energy molecules include:
- ATP, UTP, GTP: donators of phosphoryl group.
- NADH, FADH2: donators of electrons or hydrogen.
- Biotin: donator of carboxyl group.
- Acetyl CoA: donator of acyl group.
- Others: THF-C, Thpp, S-Adenosylmethionine, UDP-Glucose.
A note about enzymatic biochemistry reactions
Enzymes and substrates of a reverse reaction are usually found in a different area of the body, so forward and reverse reactions do not compete. If a two-way reaction is found in the same area, then negative (or positive) feedback of enzymes prevent a "futile cycle" (competition within two-way reactions).
ATP production
Glycolysis occurs in all organ cells, producing two pyruvates per glucose. Pyruvate is converted to acetyl CoA, which can enter the Krebs cycle. Besides glycolysis, acetyl CoA can also be formed through fatty acid degradation or by transformation of certain amino acids.
Glycolysis (cytosol)
Produces 2 pyruvate, net 2 ATP and 2 NADH per glucose.
Anaerobic glycolysis (cytosol)
The Krebs cycle needs O2 to run, otherwise anaerobic glycolysis will occur. It is like glycolysis with an extra step: cycle the 2 NADH to replenish 2 NAD+ via transformation of 2 pyruvate to 2 lactate. Net 2 ATP.
Pyruvate decarboxylation (mitochondria)
Produces 2 acetyl CoA and 2 NADH per glucose.
Krebs cycle and Oxidative phosphorylation (mitochondria)
Including pyruvate decarboxylation, the Krebs cycle produces 1 ATP, 1 GTP, 8 NADH, and 2 FADH2 per glucose. In the electron transport chain, phosphorylation (ATP production) is coupled with oxidation (requiring O2 at the end).
Based on newer sources, 2.5 ATP are generated per NADH in the mitochondria. 1.5 ATP are generated per NADH in the cytosol, and per FADH2. This is a total of 30-32 ATP per glucose in aerobic respiration.
Note that the presence of ADP stimulates oxidation, and the lack of ADP (and abundance of ATP) slows the rate of oxidation.
 |
| Cell Respiration by RegisFrey |
Connections to other processes
Glyceraldehyde 3-P (halves of glucose) can be directed back towards gluconeogenesis, or towards acetyl CoA and the Krebs cycle. Amino acids can be transformed into acetyl CoA or other molecules in the Krebs cycle, and vice versa. Acetyl CoA is also used to generate lipids (lipogenesis). Succinyl CoA can be used to produce heme molecules, while other molecules from the Krebs cycle can be used to make purines and pyrimidines for DNA synthesis.
Thursday, March 13, 2014
T Cell Education in the Thymus
 |
| Intrathymic T Cell Differentiation by Wilson Savino |
Process of T cell education
- Immature T cells from the bone marrow enter thymus via blood. T cells are "nude" and have no expression of Fas, CD4, CD8 or TCR.
- T cells migrate to the cortex, the outer region of the thymus, and proliferate.
- Some T cells start to encode α and β chains, and CD3 of the TCR complex. Later, they express both CD4 and CD8, and high levels of Fas, which receives apoptosis signals.
- MHC restriction: Using the Fas apoptotic scheme, cortical epithelial cells test positive selection for MHC recognition in T cells. (If MHC binding is too weak, then the T cell dies).
- Central tolerance induction: T cells pass to the medulla (central thymus) and test tolerance for self using negative selection. Thymic DCs that have migrated from the bone marrow present self peptides to T cells. Medullary thymic epithelial cells also test tolerance for tissue-specific peptides. (If peptide binding is too strong, then the T cell dies). T cells are now single positive for either CD4 or CD8.
Wednesday, March 12, 2014
Secondary Lymphoid Organs
Secondary lymphoid organs include lymph nodes, spleen and mucosa-associated lymphoid tissue (MALT). These structures are passages for blood and lymphatics, and possess distinct areas where T cells and B cells proliferate.
Lymph node
B cells, T cells and dendritic cells enter and exit the lymph node through the afferent and efferent lymphatic vessels, or through the blood vessels. In contrast to DCs, follicular dendritic cells (FDCs) reside within secondary lymphoid organs, and present antigen to B cells.
B cells and FDCs are found in the cortex. T cells and DCs are found in the paracortex (not labeled) towards the center of the lymph node. The cortex contains lymphoid follicles (shown in red), also known as primary lymphoid follicles. Active lymphoid follicles are called secondary lymphoid follicles or germinal centers where B cells proliferate and grow.
B cell proliferation
The germination center has a "light zone" where step 5 occurs, and a "dark zone" where steps 3 and 4 occur. It is so named because proliferated B cells move toward the edge to be nearer to Th cells, forming a darker region.
High endothelial venule
Found in the venules, where lymphocytes exit the blood into the lymph (except in the spleen). T cells return to the lymph node via the HEV to be restimulated, proliferate, and stimulate any rare B cells.
Chemokines
FDCs produce CXCL13 to attract naive B cells. B cells that have found their antigen upregulate receptor CCR7 to migrate towards the edge of the germinating center, where they will receive help from Th cells. Likewise, activated Th cells upregulate receptors to migrate towards this same region.
Peyer's patch (MALT)
This is a MALT found in the intestine, with M cells that uptake antigen into the lymphoid organ. There is no incoming lymphatic vessel.
Spleen (blood filter)
There are no lymphatics. Everything from the blood can enter and pass.
Lymph node
 |
| Structure and Histology of a Lymph Node by OpenStax College |
B cells, T cells and dendritic cells enter and exit the lymph node through the afferent and efferent lymphatic vessels, or through the blood vessels. In contrast to DCs, follicular dendritic cells (FDCs) reside within secondary lymphoid organs, and present antigen to B cells.
B cells and FDCs are found in the cortex. T cells and DCs are found in the paracortex (not labeled) towards the center of the lymph node. The cortex contains lymphoid follicles (shown in red), also known as primary lymphoid follicles. Active lymphoid follicles are called secondary lymphoid follicles or germinal centers where B cells proliferate and grow.
B cell proliferation
- In the lymphoid follicle, FDCs take in opsonized antigen. Both complement proteins and antibodies are recognized by the FDC.
- FDCs cross-link B cells and the few B cells that recognize a presented antigen stay and proliferate.
- Proliferated B cells are apoptotic unless activated Th cells migrate to the lymphoid organ and provide costimulation (CD40L).
- B cell activation. The B cell also costimulates the T cell (B7) and present antigen.
- Some B cells become plasma B cells and leave to the blood. Others undergo somatic hypermutation and cycle the lymphoid follicle again.
The germination center has a "light zone" where step 5 occurs, and a "dark zone" where steps 3 and 4 occur. It is so named because proliferated B cells move toward the edge to be nearer to Th cells, forming a darker region.
High endothelial venule
Found in the venules, where lymphocytes exit the blood into the lymph (except in the spleen). T cells return to the lymph node via the HEV to be restimulated, proliferate, and stimulate any rare B cells.
Chemokines
FDCs produce CXCL13 to attract naive B cells. B cells that have found their antigen upregulate receptor CCR7 to migrate towards the edge of the germinating center, where they will receive help from Th cells. Likewise, activated Th cells upregulate receptors to migrate towards this same region.
Peyer's patch (MALT)
This is a MALT found in the intestine, with M cells that uptake antigen into the lymphoid organ. There is no incoming lymphatic vessel.
Spleen (blood filter)
There are no lymphatics. Everything from the blood can enter and pass.
B Cell
B cell activation
T cell dependent
T cell independent (faster activation, recognizes a range of antigen other than protein)
What is clustering?
When BCRs are brought close together, internal signaling proteins are concentrated enough to begin an enzymatic chain reaction.
Activated B cells
 Fully activated B cells have the choice to undergo class switching (from IgM) or somatic hypermutation.
Fully activated B cells have the choice to undergo class switching (from IgM) or somatic hypermutation.
Class switching
Changes of the gene encoding the tail or heavy chain of the antibody affect the antibody type. This is done by the cutting and pasting of constant region segments. Remember that "VJC" is the light chain, and "VDJC" is the heavy chain.
Somatic hypermutation
"VDJ" gene segments undergo mutation at a high rate to create and circulate more fine-tuned B cells.
Antibodies
IgM
IgG
IgA
IgE
T cell dependent
- B cell receptors (BCRs) cluster by recognizing epitopes of a pathogen. To promote clustering, complement receptor type 2 (Cr2) on the B cell can anchor invaders that are opsonized by C3b, bringing the pathogen closer to the BCRs. This is an example of how the innate immune system identifies the invaders for the adaptive.
- CD40L of T cells ligate CD40 of B cells, providing the signal for cell activation. (Therefore, APCs activate T cells activate B cells).
T cell independent (faster activation, recognizes a range of antigen other than protein)
- Repeated epitopes cluster BCRs, which substitutes for CD40L costimulation.
- Battle cytokines, such as IFN-γ, fully activate B cells.
What is clustering?
When BCRs are brought close together, internal signaling proteins are concentrated enough to begin an enzymatic chain reaction.
Activated B cells

Class switching
Changes of the gene encoding the tail or heavy chain of the antibody affect the antibody type. This is done by the cutting and pasting of constant region segments. Remember that "VJC" is the light chain, and "VDJC" is the heavy chain.
Somatic hypermutation
"VDJ" gene segments undergo mutation at a high rate to create and circulate more fine-tuned B cells.
Antibodies
 |
| IgG/IgE isotype |
- First evolved aB.
- Appearance of five IgGs stuck together.
- Good at fixing complement. C1 proteins bind to the Fc region. Two C1 clusters activate the complement cascade to form C3b. This allows the complement system to direct an attack on any bacteria, even those that resist complent protein attachment.
IgG
- Unique in that it passes the placenta.
- Longest lived aB.
- Abundant in blood.
- Can fix complement with at least two IgGs, but not well.
IgA
- Most abundant in body, in mucosal linings.
- Secreted in milk.
- Has a clip that holds together two IgGs at the tail region. The clip helps transport IgA in and out of the intestine, and makes IgA resistant to acid and enzymes.
- Does not fix complement.
IgE
- Loaded onto mast cells when the body is first exposed to an allergen.
- Degranulates mast cells upon second exposure where IgE binds to the same allergen. This causes an allergic reaction.
Monday, March 10, 2014
T Cell
Antigen Presenting Cell (APC)
Dendritic cells deal with first encounters of a pathogen. Macrophages support the immune response with continued antigen presentation to T cells. B cells have a late but effective response; they are also prepared in case of a second encounter.
Helper/Killer T cell activation by APC
This describes the TCR of the most common T cell type. The components of the signaling complex are:
Dendritic cells deal with first encounters of a pathogen. Macrophages support the immune response with continued antigen presentation to T cells. B cells have a late but effective response; they are also prepared in case of a second encounter.
Helper/Killer T cell activation by APC
 |
| Antigen presentation by Sjef |
- The T cell comes in contact with an APC by weak adhesion molecules as TCR binds MHC.
- T cell upregulates CD40L, which binds CD40 on APC.
- This stimulates MHC and B7, or other costimulating molecules, on the APC. (B7 ligates CD28).
- Costimulation amplifies the TCR signal. This is important for naive T cell activation, whereas costimulation is not needed in activated T cells.
- More efficient T cell activation.
(Not shown in image). CD4 or CD8 also act like a "clip" to strengthen the adhesion of the TCR and MHC. With cytotoxic T cells, CD8 binds MHC I. With helper T cells, CD4 binds MHC II.
αβ T cell signaling
 |
| TCR Complex by Anriar |
TCR made of α and β chains, for antigen recognition. The TCR comes into contact with antigen-loaded MHC molecules.
CD3 made of four peptide chains: γ, δ and ε associate with the TCR; the ζ-chain generates an intracellular activation signal.
Th cytokines
Helper T cells respond specifically to a pathogen by producing cytokines.
Th1 (classical subset against viruses and bacteria)
- IL-2, the growth factor of CTL and NK cells. Therefore, when many CTLs are needed in a viral infection, the Th cell controls the strength of the cytotoxic T cell response.
- IFN-γ, which primes macrophages and influences IgG class switch in B cells.
- TNF, which activates macrophages and NK cells.
Th2 (parasitic or mucosal subset)
- IL-5, which encourages B cell IgA production.
- IL-10, which downregulates Th1 cytokines and enhances B cell survival and proliferation.
- IL-4, a B cell growth factor; influences IgE class switch in B cells.
Sunday, March 9, 2014
Innate Immune System, Abridged
Leukocyte extravasation
Neutrophils, eosinophils and mast cells exit the blood and enter tissues by extravasation. This begins when endothelial cells of the blood vessel express surface proteins selectin (SEL) and intercellular adhesion molecule (ICAM) in response to local cytokines IL-1 and TNF, which are produced by macrophages at the site of inflammation.
Extravasating immune cells possess ligands selectin ligand (SLIG) and integrin (INT). INT is expressed in response to inflammatory signals (for the neutrophil, the signals are LPS and complement protein C5a).
Major histocompatibility complex
MHC class I molecules are found on non-immune cells, which present cellular proteins to killer T cells. MHC class II molecules are found on immune cells, which present foreign proteins to helper T cells.
Macrophage hyperactive state
Inputs
IFN-γ received from Th cells or NK cells prime the macrophage to upregulate MHC II molecules. This lets the macrophage become an active antigen presenter to Th cells. A primed macrophage becomes hyperactive when it detects the presence of LPS or mannose.
Outputs
Hyperactive macrophages produce alarm signals IL-1 and TNF, and NK cell-activating IL-12.
Neutrophils, eosinophils and mast cells exit the blood and enter tissues by extravasation. This begins when endothelial cells of the blood vessel express surface proteins selectin (SEL) and intercellular adhesion molecule (ICAM) in response to local cytokines IL-1 and TNF, which are produced by macrophages at the site of inflammation.
Extravasating immune cells possess ligands selectin ligand (SLIG) and integrin (INT). INT is expressed in response to inflammatory signals (for the neutrophil, the signals are LPS and complement protein C5a).
- SEL and SLIG contribute to rolling adhesion.
- ICAM and INT is a strong interaction, causing the immune cell to stop rolling.
- Extravasation to the battle site.
Major histocompatibility complex
MHC class I molecules are found on non-immune cells, which present cellular proteins to killer T cells. MHC class II molecules are found on immune cells, which present foreign proteins to helper T cells.
Macrophage hyperactive state
Inputs
IFN-γ received from Th cells or NK cells prime the macrophage to upregulate MHC II molecules. This lets the macrophage become an active antigen presenter to Th cells. A primed macrophage becomes hyperactive when it detects the presence of LPS or mannose.
Outputs
Hyperactive macrophages produce alarm signals IL-1 and TNF, and NK cell-activating IL-12.
- TNF kills tumor cells and virus-infected cells, and activates immune cells, including the macrophage to produce IL-12.
- Neutrophils also produce TNF, as they are one of the first responders to inflammation.
Natural Killer cell
Inputs
The detection of LPS causes NK cells to produce IFN-γ; the production of IFN-γ is increased by signals IL-12 and TNF. TNF also influences the upregulation of IL-2R in NK cells.
Outputs
NK cells produce the growth factor IL-2. When there is an increase of IL-2 receptors, NK cells will proliferate.
Inputs
The detection of LPS causes NK cells to produce IFN-γ; the production of IFN-γ is increased by signals IL-12 and TNF. TNF also influences the upregulation of IL-2R in NK cells.
Outputs
NK cells produce the growth factor IL-2. When there is an increase of IL-2 receptors, NK cells will proliferate.
- NK cells destroy virus-infected cells if a combination of signals exists: MHC I and an unusual surface protein or carbohydrate. However, if there is a high balance of MHC I, the NK cell determines that the cell is healthy and does not destroy the cell.
Dendritic cell
Inputs
DC cells become activated in response to TNF or antigen recognition by their toll-like receptors (TLR). Chemokines encourage extravasation.
Inputs
DC cells become activated in response to TNF or antigen recognition by their toll-like receptors (TLR). Chemokines encourage extravasation.
- The activated DC cell uptakes tissue antigens to load onto MHC II molecules, and expresses MHC II on the cell surface. When it travels to the nearest lymph node, it upregulates surface protein B7 and MHC I (in the event the DC cell may be infected).
- In the lymph node, DC cells act as antigen presenters and T cell activators. B7 pairs with CD28 on the T cell, and MHC pairs with T cell receptors (TCRs).
Complement pathways
Alternate (non-discriminate binding)
- C3 made by liver to blood.
- Spontaneous: C3 → C3a + C3b
- C3b binds to cell surface.
- C3b + B → C3bB
- C3bB + D (cleaver) → C3bBb
- Propagation: C3 + C3bBb (cleaver) → C3b → → C3bBb
- C5 + C3bBb (cleaver) → C5b
- C5b + C6 + C7 + C8 + C9 → MAC
Classical (occurs with two units of IgG or IgM; only the pathogen is targeted)
- Antibody binds antigen.
- Two activated subunits C1s form a C1 complex at the Fc tail.
- C2 + C1s (cleaver) → C2a + C2b
- C4 + C1s (cleaver) → C4a + C4b
- Forms on pathogen surface: C4b + C2b → C4b2b
- C3 + C4b2b (cleaver) → C3a + C3b
- Step 3 of Alternate.
Lectin (MBL only binds pathogenic carbohydrate)
- MBL made by liver to blood.
- MBL + MASPs
- MBL/MASP complex binds to pathogen surface.
- C3 + MASP (cleaver) → C3a + C3b
- Step 3 of Alternate.
Wednesday, February 26, 2014
Digestive System
Vagus nerve and motility
One function of the vagus nerve is to stimulate digestion by GI secretion and peristalsis throughout the digestive tract. The vagal nerve fiber myenteric plexus influences motility, and is strategically located between the circular and longitudinal muscle layers. The Meissners' plexus influence secretion and lies near the glandular regions.
Digestion and absorption
Carbohydrates are broken down to monosaccharides in the mouth, and are absorbed in the small intestine. intestine and pancreas. Intestinal and pancreatic glands secrete enzymes that also hydrolyze starches. (Different intestinal and pancreatic enzymes digest carbohydrate, protein and fat).
Protein digestion begins in the stomach and ends in the small intestine, where proteins are broken down to amino acids and small peptides.
Fat is emulsified, or broken into small droplets, by the stomach. Triglycerides, cholesterol esters and phospholipids are broken down in the intestine, and then combine with bile salts to form micelles. Micelles carry the digested lipid products to be absorbed into the intestinal epithelial cell, where the triglycerides, cholesterol esters and phospholipids are reformed. These molecules are combined with apoproteins to form chylomicrons, which exit the cell into the lymphatics.
Chylomicrons travel to the liver, where by further processing, they become lipoprotein vehicles VLDL, LDL, IDL or HDL. Triglycerides are most concentrated in VLDL, which is transported to fat, skeletal and heart muscle cells. Cholesterol is found in all lipoprotein vehicles, but is most concentrated in LDL and HDL.
Table of digestive chemicals
One function of the vagus nerve is to stimulate digestion by GI secretion and peristalsis throughout the digestive tract. The vagal nerve fiber myenteric plexus influences motility, and is strategically located between the circular and longitudinal muscle layers. The Meissners' plexus influence secretion and lies near the glandular regions.
Digestion and absorption
 |
| Micelle scheme by SuperManu |
Protein digestion begins in the stomach and ends in the small intestine, where proteins are broken down to amino acids and small peptides.
| Chylomicron illustration by OpenStax College |
Chylomicrons travel to the liver, where by further processing, they become lipoprotein vehicles VLDL, LDL, IDL or HDL. Triglycerides are most concentrated in VLDL, which is transported to fat, skeletal and heart muscle cells. Cholesterol is found in all lipoprotein vehicles, but is most concentrated in LDL and HDL.
Table of digestive chemicals
| Organ | Cell type | Produces | Function |
| Mouth | Salivary gland | Salivary amylase | Partially breaks down starch. |
| Stomach | Chief cell (Stimulated by gastrin, pepsin and HCl). | Pepsinogen | In the presence of acid, changes to pepsin and break down proteins to peptides. |
| Parietal cell (Stimulated by vagus, gastrin, stomach stretch and presence of peptides. Inhibited by acidity, secretin, GIP, somatostatin and cholecystokinin). | HCl | Creates an acidic environment for pepsin, and has a small effect on starch hydrolysis. | |
| Intrinsic factor | Binds to vitamin B12 to aid its absorption in the small intestine. | ||
| Gastrin cell (Stimulated by vagus, duodenum stretch and presence of peptides. Inhibited by acidity, secretin and GIP). | Gastrin | Stimulates parietal cell to secrete HCl, and increases intestinal motility. | |
| Duodenum / Small intestine | Epithelial cells of Crypts of Lieberkuhn (Stimulated by vagus and direct contact with food. Secretin, GIP and cholecystokinin secretion are stimulated by fat and acid). | Maltase, Lactase, Sucrase | Splits maltose to glucose, lactose to glucose and galactose, and sucrose to glucose and fructose, respectively. |
| Peptidase | Breaks down peptides to amino acids. | ||
| Intestinal lipase, Intestinal enterase | Breaks down fats to glycerol and fatty acids, and cholesterol esters to free cholesterol and fatty acids, respectively. | ||
| Secretin, Gastric inhibitory peptide (GIP), Cholecystokinin | Decrease gastrin secretion and motility. | ||
| Enterokinase | A catalyst for the activation of pancreas peptides: trypsinogen, chymotrypsinogen, and procarboxypolypeptidase. | ||
| Pancreas (exocrine) | Exocrine cell (Stimulated by vagus, cholecystokinin and secretin). | Trypsinogen, Chymotrypsinogen, Procarboxypolypeptidase | Break down proteins to peptides and amino acids. |
| Pancreatic lipase, Cholesterol esterase, Phospholipase | Breaks down triglycerides to fatty acids and monoglycerides, cholesterol esters to free cholesterol and fatty acids, and phospholipids to lysophospholids and fatty acids, respectively. | ||
| Pancreas (endocrine) | Beta islet cell | Insulin | Increases intestinal motility. |
| Alpha islet cell | Glucagon | Decreases intestinal motility. | |
| Delta islet cell | Somatostatin | Decreases digestion and absorption, and insulin and glucagon secretion. | |
| Liver | Liver cell | Bile salt | Emulsifies fat to smaller particles that can be digested by pancreatic enzymes. |
Monday, February 24, 2014
Mechanoreceptors and Muscle Contraction
 |
| Sarcomere by Sameerb |
Mechanoreceptors
Golgi tendon organs detect tension in muscle tendons. Muscle spindles lie within the center of a muscle, and detect stretch.
These receptors provide continuous feedback on the degree of muscle stretch and tension and the speed of stretching in order to achieve smooth and precise muscle action.
Muscle spindle
The two sensory receptors of muscle spindles are called primary and secondary nerve endings. They relay information about the degree of muscle stretching. Primary nerve endings also detect the rate of muscle stretching.
If a muscle remains stretched, the receptors send negative feedback information to the spinal cord and cerebellum, causing muscle contraction. If a muscle is suddenly stretched, then the primary receptors provide additional strong input to the spinal cord. An example is the knee jerk reflex.
Muscle spindles also consist of extrafusal muscle fibers (stimulated by gamma motor neurons), and smaller intrafusal muscle fibers (alpha motor neurons). Gamma motor neurons fire whenever alpha motor neurons fire, ensuring the length of intrafusal fibers and extrafusal fibers keep pace in contraction.
Golgi tendon organ
The Golgi tendon organ reacts against increased muscle tension by decreasing tension (allowing muscle to stretch).
Muscle contraction (animation)
- An action potential spreads through the muscle fiber's T-tubules network.
- Depolarization of the muscle fiber eventually causes the sarcoplasmic reticulum to release calcium.
- The calcium binds to the actin filament (on troponin C), causing an allosteric change of troponin and allowing tropomyosin to move. The binding site is unblocked. When calcium is present the blocked active site of the actin clears.
- Myosin binds to the binding site on the thin filament, releasing phosphate and then ADP. (The myosin head has ADP and Pi attached in its high energy configuration).
- The release of ADP is coupled to the power stroke, where the myosin head pivots and pulls the actin filament toward the center.
- ATP binds to myosin head, allowing it to release actin and be in the weak binding state. The lack of ATP results in the rigor state characteristic of rigor mortis.
- ATP is split into ADP and Pi by hydrolysis.
- Steps 4 to 7 repeat as long as ATP is available and calcium is freely found within the thin filaments.
- Meanwhile, calcium is actively pumped back into the sarcoplasmic reticulum. When calcium is no longer present on the thin filament, the tropomyosin changes conformation back to its previous state, and blocks the binding site again. The myosin ceases binding to the thin filament, and the contractions cease.
Neuronal Circuitry
The postsynaptic neuron adds together the simultaneous firings of its presynaptic neurons until threshold. The axon hillock of the postsynaptic neuron then generates the action potential.
Temporal summation
The postsynaptic neuron receives rapid and frequent action potentials from few presynaptic neurons. Excited neurons have a greater effect on the postsynaptic neuron, causing the axon hillock to generate an action potential.
Neurotransmitters
Neurotransmitters that depolarize the postsynaptic neuron cause excitatory postsynaptic potentials (EPSPs). Neurotransmitters that inhibit the neuron from firing cause inhibitory postsynaptic potentials (IPSPs).
Acetylcholine, norepinephrine and glutamate are mostly excitatory. Dopamine, gamma-aminobutyric acid (GABA), glycine and serotonin are mostly inhibitory.
Neuronal circuitry
- Convergence: a neuron takes in multiple inputs.
- Divergence: a neuron outputs to multiple cells.
- Negative feedback: neuron A stimulates neuron B that inhibits the outputs of neuron A.
- Lateral inhibition: a neuron stimulates its postsynaptic neurons, which send inhibitory signals and only a few excitatory signals. This limits neural impulses to a narrow path.
- Reverberation: a positive feedback circuit to sustain firing along a neural pathway.
Thursday, February 20, 2014
Blood Cells and Blood Clotting
Stimulus of RBC production
Decreased blood oxygen (anemia) stimulates erythropoietin production by the kidneys, a hormone that stimulates RBC production.
Factors of RBC effectiveness
- RBC production in the marrow. Radiation or drugs may suppress the marrow and decrease the number of RBCs.
- Iron in the diet to produce the hemoglobin molecule. An iron deficiency causes anemia.
- Vitamin B12 and folic acid, important in the synthesis of DNA and the development of RBCs in the bone marrow. A deficiency of either will lead to megaloblastic anemia, where cells are large, fragile and short-lived.
- Defects in the structure of hemoglobin may cause anemia. For example, sickle cell anemia.
- Defects in the red cell membrane.
- Defect in the metabolic pathway of RBCs.
- Immune reaction against RBCs, especially due to the cell defects above.
Platelets
Platelets are small, anuclear cell fragments responsible for blood clotting. They secrete ADP and thromboxane A2 to activate other platelets to become "sticky". They also produce a fibrin-stabilizing factor that binds fibrin molecules to strengthen and form the clot, and prostaglandins that have various effects on blood flow and wound healing. They possess actin and myosin that allow them to retract and help close damaged blood vessel. The glycoprotein Von Willenbrand factor is the initial bridge that connects platelets to injured vessel wall.
Blood clotting
- Severed blood vessel causes local blood vessels to constrict.
- Extrinsic or Intrinsic pathway:
- Extrinsic is a quick response triggered by tissue trauma releasing tissue thromboplastin.
- Intrinsic is a slow reaction triggered by damage to RBCs, or by RBC contact with a foreign surface.
- Formation of prothrombin activator.
- Prothrombin activator catalyzes prothrombin to thrombin.
- Thrombin changes fibrinogen to fibrin threads that mix with RBCs, platelets and plasma to form a clot.
- Clot retraction and healing.
Negative feedback mechanisms of blood clotting
- Fibrin absorbs excess thrombin, preventing the formation of more fibrin.
- A globulin called anti-thrombin III inactivates excess thrombin. Heparin, produced by mast cells and basophils, is an anti-coagulant that works by enhancing anti-thrombin III activity.
- Tissue plasminogen activator, released from damaged tissues, activates plasma protein plasminogen (profibrinolysin) to become plasmin (fibrinolysin). Plasmin lyses fibrin and helps remove the clot.
Diseases of clotting
- Von Willenbrand's disease, caused by a defect in plasma adhesion and results in prolonged bleeding.
- Hemophilia A and B are caused by missing Factor VIII and Factor IX, respectively.
- Bleeding problems caused by vitamin K deficiency. Vitamin K is important in the formation of prothrombin and factors VII, IX and X.
Wednesday, February 19, 2014
Respiratory System
Carbon dioxide in the body
CO2 combines with water to form H2CO3 in the RBC, catalyzed by enzyme carbonic anhydrase. H+, from H2CO3, combines with hemoglobin (protein buffer) and HCO3- leaves the cell into plasma. When the RBC reaches the lungs, its hemoglobin releases H+ and H+ combines with a bicarbonate ion to reform CO2.
Oxygen in the body
 Unlike carbon dioxide, oxygen is not very soluble in plasma, but is carried on the hemoglobin of RBCs. In the oxygen-hemoglobin dissociation curve, hemoglobin easily gives up oxygen to tissues where there is low pO2 (40 mmHg), yet binds well to oxygen in the alveoli where there is high pO2 (60-100 mmHg). Hemoglobin also releases more O2 when pCO2 is elevated, when pH is low, or when temperature is high (where oxygen needs may be increased). This is represented by the dissociation curve shifting right, for reduced affinity.
Unlike carbon dioxide, oxygen is not very soluble in plasma, but is carried on the hemoglobin of RBCs. In the oxygen-hemoglobin dissociation curve, hemoglobin easily gives up oxygen to tissues where there is low pO2 (40 mmHg), yet binds well to oxygen in the alveoli where there is high pO2 (60-100 mmHg). Hemoglobin also releases more O2 when pCO2 is elevated, when pH is low, or when temperature is high (where oxygen needs may be increased). This is represented by the dissociation curve shifting right, for reduced affinity.
How do cells control the use of oxygen?
The level of ADP limits O2 consumption. This means when ADP is low (and there is abundant ATP), the cell doesn't need as much O2. Less O2 reacts in oxidative phosphorylation to produce ATP.
How does the brain control respiration?
Carbon dioxide and H+
Increased blood CO2 or H+ level stimulate the brain stem to increase respiration in order to remove excess CO2 and decrease blood acidity. Carotid and aortic bodies are also stimulated to increase firing, which relays neural messages to the brain stem to increase respiration.
Oxygen
Decreased blood pO2 increases the firing of the carotid and aortic bodies. This information is relayed to the brain stem.
Hering-Breuer reflex
Stretch in the lungs at the bronchiolar and bronchial tree tells the brain stem to inhibit inspiration.
Note: Remember that the CO2 control mechanism also balances blood pH. The O2 control mechanism is simple and does no more than balancing O2 level.
Respiratory problems
Inspiratory muscles / Control of respiration
Examples: brain stem injury, spinal cord injury, stroke, polio.
Pneumothorax
Air wrongly enters into pleural space, causing lung collapse due to inadequate negative pressure. Causes include obstruction of respiratory passage, thick membrane preventing efficient gas diffusion (pulmonary edema), fluid in alveolar space (pulmonary edema, pneumonia).
Diminished surface area of alveolar space from damage
Examples: collapsed alveoli (atelectasis), scarring of the lung (pulmonary fibrosis), alveolar destruction from smoking (emphysema).
Abnormally low blood oxygen (arterial hypoxemia)
Oxygen fails to diffuse into the lungs, due to low air ventilation or poor blood perfusion at the alveolar membrane.
Inefficient cardiovascular perfusion of tissues
Oxygen supply cannot meet the tissue energy needs during intense exercise.
Respiratory effort terminology
CO2 combines with water to form H2CO3 in the RBC, catalyzed by enzyme carbonic anhydrase. H+, from H2CO3, combines with hemoglobin (protein buffer) and HCO3- leaves the cell into plasma. When the RBC reaches the lungs, its hemoglobin releases H+ and H+ combines with a bicarbonate ion to reform CO2.
Oxygen in the body

How do cells control the use of oxygen?
The level of ADP limits O2 consumption. This means when ADP is low (and there is abundant ATP), the cell doesn't need as much O2. Less O2 reacts in oxidative phosphorylation to produce ATP.
How does the brain control respiration?
Carbon dioxide and H+
Increased blood CO2 or H+ level stimulate the brain stem to increase respiration in order to remove excess CO2 and decrease blood acidity. Carotid and aortic bodies are also stimulated to increase firing, which relays neural messages to the brain stem to increase respiration.
Oxygen
Decreased blood pO2 increases the firing of the carotid and aortic bodies. This information is relayed to the brain stem.
Hering-Breuer reflex
Stretch in the lungs at the bronchiolar and bronchial tree tells the brain stem to inhibit inspiration.
Note: Remember that the CO2 control mechanism also balances blood pH. The O2 control mechanism is simple and does no more than balancing O2 level.
Respiratory problems
Inspiratory muscles / Control of respiration
Examples: brain stem injury, spinal cord injury, stroke, polio.
Pneumothorax
Air wrongly enters into pleural space, causing lung collapse due to inadequate negative pressure. Causes include obstruction of respiratory passage, thick membrane preventing efficient gas diffusion (pulmonary edema), fluid in alveolar space (pulmonary edema, pneumonia).
Diminished surface area of alveolar space from damage
Examples: collapsed alveoli (atelectasis), scarring of the lung (pulmonary fibrosis), alveolar destruction from smoking (emphysema).
Abnormally low blood oxygen (arterial hypoxemia)
Oxygen fails to diffuse into the lungs, due to low air ventilation or poor blood perfusion at the alveolar membrane.
Inefficient cardiovascular perfusion of tissues
Oxygen supply cannot meet the tissue energy needs during intense exercise.
Respiratory effort terminology
- Tidal Volume (TV), the average breath of air inhaled or exhaled.
- Inspiratory Reserve Volume (IRV), the extra amount of air that can be inhaled after TV.
- Expiratory Reserve Volume (ERV), the extra amount of air that can be exhaled after TV.
- Residual Volume (RV), the air left in lungs after strongest expiration.
- Functional Residual Capacity (FRC) = RV + ERV. (After TV exhalation, the total remaining volume of air in the lungs).
- Inspiratory Capacity (IC) = TV + IRV. (After TV exhalation, the maximal volume of air that can be inhaled).
- Vital Capacity (VC), the maximum amount of air you can ever inhale or exhale, an exchange between maximal intake and most forceful expiration.
- Total Lung Capacity (TLC), maximal volume of air in the lungs (after maximal inhalation).
Tuesday, February 18, 2014
Acid-Base Physiology
Hydrogen regulation
Depletion of chloride and K+ from the blood causes H+ loss
Depletion of chloride and K+ from the blood causes H+ loss
H+ is secreted into the renal tubule lumen, causing metabolic alkalosis. Specifically, chloride loss is accompanied by H+ to preserve charge (rather than Na+, which cannot accompany chloride in reabsorption). K+ loss decreases aldosterone release to allow more K+ into the blood. K+ is secreted into the plasma in exchange with H+ into the cell.
Sodium depletion of the blood causes H+ loss
Buffering systems: HB ↔ H+ + B-
Sodium depletion of the blood causes H+ loss
Low Na+ causes more aldosterone to be secreted, and it stimulates potassium loss, which in turn stimulates H+ secretion in the same mechanism above. Another reason is that sodium depletion causes increased sodium reabsorption into the blood, where H+ exchanges for sodium during reabsorption and there is increased H+ secretion into the renal tubules.
Buffering systems: HB ↔ H+ + B-
A common system involves a weak acid (HB), a strong acid (H+) and a weak conjugate base (B-). The addition of a strong acid or base is partially neutralized by B- or H+, and does not drastically change the pH.
- Bicarbonate buffer: (CO2 + H2O) ↔ H2CO3 ↔ H+ + HCO3-
- The main extracellular buffering system.
- Addition of a strong acid will shift the equation to the left, whereas strong base to the right.
- To restore pH, the lungs may expire carbon dioxide and decrease blood acidity. The kidneys decrease blood acidity by secreting bicarbonate (which, in the acidotic state, is in lowered concentrations) to the blood, and excreting H+.
- Phosphate and ammonia buffers: H2PO4- ↔ H+ + HPO4-2, NH4+ ↔ H+ + NH3
- Phosphate is an intracellular buffer, ammonia is an extracellular buffer.
- Using these buffers, excess H+ can be neutralized and excreted as a weak acid.
- Protein buffer: H-protein (weak acid) ↔ H+ + protein (weak conjugate base)
- An intracellular buffering system.
Respiratory acidosis
May occur in advanced pulmonary disease, where lungs do not adequately remove carbon dioxide, and the blood becomes acidic. The kidney may compensate by reabsorbing more bicarbonate to the blood.
Metabolic acidosis
The addition of an acid to the body, other than carbonic acid, or the loss of bicarbonate from the body. Bicarbonate is markedly decreased. The body responds by increasing respiration to remove carbon dioxide.
Respiratory alkalosis
Too much carbon dioxide is removed by respiration. The kidneys compensate by excreting more bicarbonate.
Metabolic alkalosis
An increase in plasma bicarbonate causes the body to decrease respiratory activity and preserve carbon dioxide.
Monday, February 17, 2014
Electrolyte Balance
| Kidney Nephron by Holly Fischer Line divides cortex (light) and medulla (dark). |
- Filtration occurs at the glomerulus, where the negatively charged, sieve-like glomerular membrane filters out molecules that are large and negatively charged.
- Reabsorption occurs in the renal tubules (the majority at the proximal convoluted tubule). Nonpolar molecules are easily reabsorbed while ions are likely to be excreted. However, sodium is actively reabsorbed into the blood by co-transporters to power the transportation of other ions.
- Secretion occurs in the renal tubules, where unfiltered molecules in the blood may still be secreted into the tubular lumen to be excreted or reabsorbed.
- The kidney produces renin, bicarbonate, prostaglandin and erythropoietin, among other molecules.
Loop of Henle, which direction?
Water reabsorption occurs in the descending limb. Think waterfall and water splashing out of the loop. Sodium reabsorption occurs in the ascending limb, which is also impermeable to water. This creates an interstitial environment that is "very salty" or hyperosmolar, and where water permeability is increased by ADH. Therefore, ADH enables water to leave the collecting ducts and concentrates urine.
Regulation of sodium
Ingestion
The hypothalamus induces "thirst" if sodium concentration is high.
Excretion
There are two autoregulatory processes. In glomerular-tubular balance, the glomerular filtration rate (GFR) influences how much sodium is filtered, and therefore, how much of (the same amount of) sodium is reabsorbed. In tubulo-glomerular feedback, the macula densa senses excessive fluid flow, which is reflected in increased GFR, and constricts the afferent arterioles to decrease GFR.
Hormone atrial natriuretic factor (ANF) responds to excessive blood volume and cardiac atria dilation, and induces sodium excretion. ADH responds to increased sodium concentrations in the blood, and conserves water to restore normal serum osmolality.
To avoid charge buildup, sodium cations must be transported with an anion, or be exchanged with a cation, such as K+ or H+. Examples: in the late proximal tubule, Na+ is reabsorbed with Cl-; in the ascending loop of Henle, the Na+-K+-2Cl- cotransporter reabsorbs these ions into the cell.
 |
| Collecting duct by Lennert B (edited) |
Potassium is the main intracellular cation, and the Na+/K+-ATPase pump keeps potassium in cells. Aldosterone stimulates the pump to take K+ into the cell and Na+ into the blood. In times of low plasma sodium, low blood pressure or high plasma potassium, aldosterone facilitates Na+ into the tubule cells (and into the blood via Na+/K+-ATPase) while K+ is excreted.
pH change
When blood pH decreases (and [H+] increases) H+ tends to enter cells in exchange for K+. When pH increases H+ tends to leave cells in exchange for K+.
Regulation of chloride
The most common extracellular anion, and is exchanged with anion bicarbonate or is carried with sodium.
pH change
When blood pH decreases (and [H+] increases) H+ tends to enter cells in exchange for K+. When pH increases H+ tends to leave cells in exchange for K+.
Regulation of chloride
The most common extracellular anion, and is exchanged with anion bicarbonate or is carried with sodium.
Friday, February 14, 2014
Circulatory Control
Autoregulation
The brain, heart and skeletal muscle exhibit autoregulatory control over their blood vessels (as opposed to blood vessels of organs under sympathetic nerve innervation). This control is based on the metabolism of surrounding tissues, and regulates blood flow locally; If there are factors such as carbon dioxide, lactic acid or certain ions, then the blood vessels will dilate. Conversely, excess blood flow will trigger vasoconstriction.
Regulation by the nervous system
Brain stem
The brain stem fires sympathetic nerve messages, and the sympathetic nerves release norepinephrine only. Sympathetic nerves also stimulate the adrenal medulla to secrete epinephrine and norepinephrine. The overall effects are raised blood pressure and increased heart rate in response to blood pressure changes.
Hypothalamus
The hypothalamus releases ADH, which increases water reabsorption in kidneys and also constricts peripheral blood vessels.
How are changes in blood pressure detected?
Juxtaglomerular apparatus and renin-angiotensin-aldosterone pathway
The brain, heart and skeletal muscle exhibit autoregulatory control over their blood vessels (as opposed to blood vessels of organs under sympathetic nerve innervation). This control is based on the metabolism of surrounding tissues, and regulates blood flow locally; If there are factors such as carbon dioxide, lactic acid or certain ions, then the blood vessels will dilate. Conversely, excess blood flow will trigger vasoconstriction.
Regulation by the nervous system
Brain stem
The brain stem fires sympathetic nerve messages, and the sympathetic nerves release norepinephrine only. Sympathetic nerves also stimulate the adrenal medulla to secrete epinephrine and norepinephrine. The overall effects are raised blood pressure and increased heart rate in response to blood pressure changes.
| Receptor | Response to | Location | Effect |
| alpha-1 | epinephrine and norepinephrine | peripheral blood vessels | vasoconstriction |
| beta-1 | norepinephrine and sympathetic nerves | heart muscle | increase cardiac output |
| alpha-2 | norepinephrine | presynaptic terminals of CNS | negative feedback inhibiting norepinephrine release |
| beta-2 | epinephrine | blood vessels of the skeletal muscle and heart | vasodilation |
Hypothalamus
The hypothalamus releases ADH, which increases water reabsorption in kidneys and also constricts peripheral blood vessels.
How are changes in blood pressure detected?
- If blood pressure is too high, baroceptors in the carotid and aortic sinuses (vessels in the upper body) fire signals that inhibit sympathetic output.
- The hypothalamus responds to increased serum osmolality (mainly increases of sodium in the blood) by secreting more ADH.
- The brain stem responds to increased concentrations of blood CO2 and H+, which are associated with low blood pressure and poor blood flow, by stimulating sympathetic output.
Regulation by the kidney
Glomerular level
Water filtration at the glomerulus depends on the hydraulic pressure and osmotic pressure of blood. The higher the hydraulic pressure, the more easily blood will pass through filtration to be secreted. The higher the osmotic pressure, the more amount of water in the blood that can be filtered.
During filtration, plasma osmolality is higher in the vessels because blood is more concentrated with proteins that do not pass into the nephron. Water tends to be drawn back into the blood due to osmotic pressure (to reach equilibrium). Thus, one must consider osmotic pressure with hydraulic pressure to determine how much water is filtered.
ADH and angiotensin II (from the renin pathway) stimulate mesangial cells in the glomerular capsule to contract. This decreases surface area and membrane permeability and more water is retained.
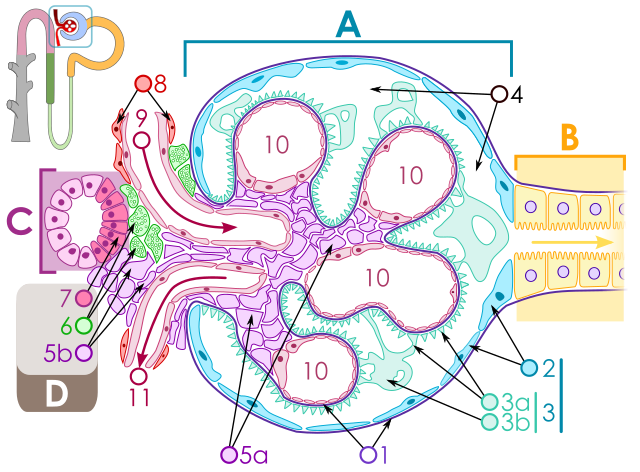 |
| Renal corpuscle by M.Komorniczak A: Renal corpuscle. B: Proximal tubule. C: Distal convoluted tubule. D: Juxtaglomerular apparatus. 5: Mesangium 6: Granular cells. 7: Macula densa. (Note the location in the nephron, upper left diagram). |
Juxtaglomerular apparatus and renin-angiotensin-aldosterone pathway
Three ways to stimulate renin secretion:
- Granular cells of the juxtaglomerular apparatus secrete renin in response to sympathetic stimulation.
- Granular cells secrete renin directly in response to low blood pressure.
- If renal tubular fluid is low in sodium, the macula densa stimulates granular cells to secrete renin. Low sodium in the renal tubules is typically the result low blood volume and slow fluid filtration, which allows too much sodium to be reabsorbed into the blood as filtrate moves too slowly.
Regulation by the heart
Atrial natriuretic factor (ANF)
Stretching of the atrial walls (by increased blood volume) releases ANF, which promotes sodium secretion and therefore loss of water. This results in lower blood volume and pressure.
Sterling's Law
Greater cardiac stretch or stroke volume = greater cardiac contraction, an automatic response to match heart input and output.
Autoregulation
See top.
Thursday, February 13, 2014
Blood Pressure and Flow
Systolic/Diastolic
Blood pressure is written as the pressure in the brachial artery as the ventricles contract (systolic) over the pressure when the ventricles relax (diastolic).
Pressure difference drives blood flow
BP is highest in the arteries, and is lowest in the veins. The pressure drop is caused by resistance as blood passes from the arteries through the capillaries. The difference in pressure is what drives blood flow (perfusion).
Factors of blood pressure
BP is controlled by volume and flow resistance. If blood volume increases, so does cardiac output (L/min) and BP. Peripheral resistance can be caused by increased blood viscosity or vasoconstriction in the arteriolar level; the resulting backup of blood in the arteries causes BP to increase.
Sympathetic nerve innervation causes vasoconstriction in blood vessels (of certain organs) with vasoconstrictive receptors.
Factors of blood flow
Of the heart:
Cardiac output is influenced by contractile force, heart rate, and venous return to the heart. Increased venous return is dependent on increased: blood volume, dilation of arteries, differential pressure between arteries and veins, skeletal muscle contractions which move blood along veins.
Of the peripheral tissues:
Increased flow is dependent on increased: cardiac output (except in coronary arteries which feed to heart muscle - a systole also contracts these arteries, blocking some flow), blood volume, vessel dilation, time spent lying down.
Also see the Poiseuille equation for factors affecting flow (Q), noting what is directly or inversely proportional to Q.
Blood pressure is written as the pressure in the brachial artery as the ventricles contract (systolic) over the pressure when the ventricles relax (diastolic).
Pressure difference drives blood flow
BP is highest in the arteries, and is lowest in the veins. The pressure drop is caused by resistance as blood passes from the arteries through the capillaries. The difference in pressure is what drives blood flow (perfusion).
Factors of blood pressure
BP is controlled by volume and flow resistance. If blood volume increases, so does cardiac output (L/min) and BP. Peripheral resistance can be caused by increased blood viscosity or vasoconstriction in the arteriolar level; the resulting backup of blood in the arteries causes BP to increase.
Sympathetic nerve innervation causes vasoconstriction in blood vessels (of certain organs) with vasoconstrictive receptors.
Factors of blood flow
Of the heart:
Cardiac output is influenced by contractile force, heart rate, and venous return to the heart. Increased venous return is dependent on increased: blood volume, dilation of arteries, differential pressure between arteries and veins, skeletal muscle contractions which move blood along veins.
Of the peripheral tissues:
Increased flow is dependent on increased: cardiac output (except in coronary arteries which feed to heart muscle - a systole also contracts these arteries, blocking some flow), blood volume, vessel dilation, time spent lying down.
Also see the Poiseuille equation for factors affecting flow (Q), noting what is directly or inversely proportional to Q.
Friday, February 7, 2014
Mycoplasma
Mycoplasmatacae are the tiniest free-living organisms capable of replicating. They are unique bacteria because they lack cell walls, having only cell membrane with sterols for protection from the environment. The lack of a cell wall explains why penicillin and other antibiotics do not attack mycoplasmatacae. Two pathogenic species are Mycoplasma pneumoniae and Ureaplasma urealyticum.
Mycoplasma pneumoniae
It is the leading cause of bronchitis and pneumonia in young adults. The mild symptoms of gradual fever, sore throat and cough is called walking pneumonia. However, it is unknown why 7% of infected patients develop severe symptoms of erythema multiforme or Stevens-Johnson syndrome.
Ureaplasma urealyticum
Found in urine and breaks down urea. It is part of normal flora in 60% of sexually active women. It can infect the lower urinary tract, causing non-gonococcal urethritis.
Mycoplasma pneumoniae
It is the leading cause of bronchitis and pneumonia in young adults. The mild symptoms of gradual fever, sore throat and cough is called walking pneumonia. However, it is unknown why 7% of infected patients develop severe symptoms of erythema multiforme or Stevens-Johnson syndrome.
Ureaplasma urealyticum
Found in urine and breaks down urea. It is part of normal flora in 60% of sexually active women. It can infect the lower urinary tract, causing non-gonococcal urethritis.
Thursday, February 6, 2014
Mycobacteria
These bacteria are rods that have high lipid content in their cell walls, which makes them acid-fast on staining. (Red stain is applied and heated to penetrate bacteria, acid alcohol is poured over the smear, then a counter stain methylene blue is applied). Mycobacteria are stained red as their cell walls do not wash off with acid alcohol, thereby retaining the first stain. Mycobacteria and Nocardia are two major acid-fast organisms.
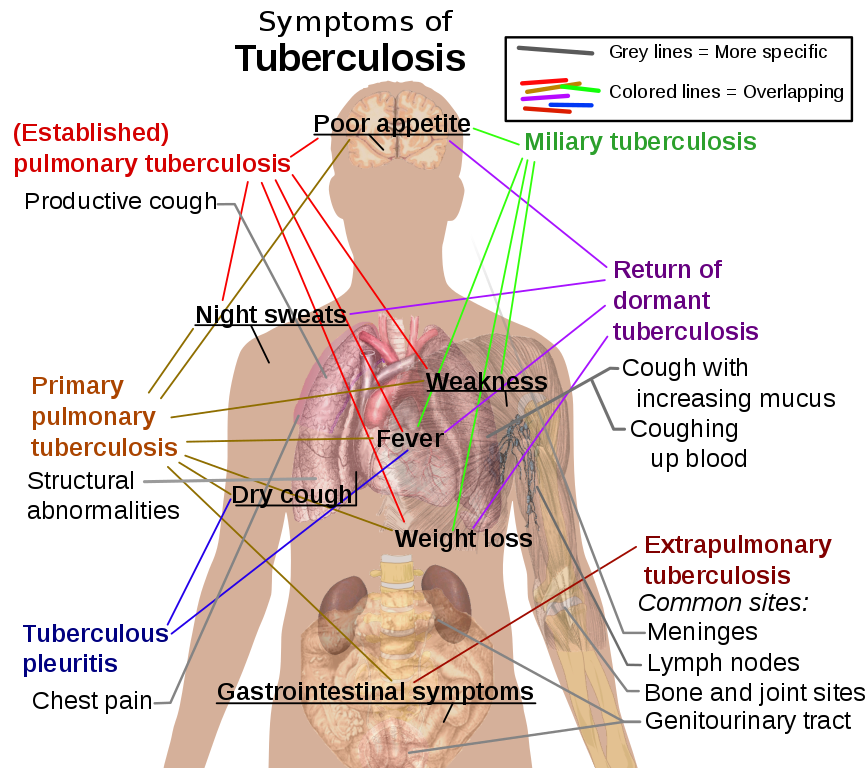
Mycobacterium tuberculosis
Commonly infects the lungs, causing the chronic disease tuberculosis. These bacteria possess mycosides, lipids that are only present in acid-fast organisms, which are involved in virulence. The formula of a mycoside is a mycolic acid bound to a carbohydrate.

Mycobacterium tuberculosis
Commonly infects the lungs, causing the chronic disease tuberculosis. These bacteria possess mycosides, lipids that are only present in acid-fast organisms, which are involved in virulence. The formula of a mycoside is a mycolic acid bound to a carbohydrate.
- Mycosides:
- Cord factor - formed by two mycolic acids and a disaccharide.
- Sulfatide - like cord factors, but sulfates are attached to the disaccharide.
- Wax D - complex mycoside that activates the immune system.
- Stages of tuberculosis:
- In primary tuberculosis, inhaled bacteria infect the lung, but is usually asymptomatic. Bacteria enter macrophages and then lymphatics and other areas of the body. Cell-mediated immunity will suppress the bacteria, but they can cause secondary tuberculosis.
- Secondary or reactivation tuberculosis occurs after the bacteria lie dormant. Infection can occur in any organ.
Mycobacterium leprae
An acid-fast, rod bacterium. Causes leprosy as it grows on the skin, preferring cooler body temperatures. This is why warm areas such as the armpit and groin are spared. Disease severity depends on one's immune system.
- Diseases:
- Lepromatous leprosy (LL), where the lack of cell-mediated immune response in patients causes leprosy in its the severest form. The reason may be due to defective T-suppressor cells that block Th cell response to the bacteria.
- Tuberculoid leprosy (TL), a milder form of leprosy as there is cell-mediated immune response against the bacteria.
Wednesday, February 5, 2014
Spirochetes (Gram-Negative)
 |
| Treponema pallidum |
Treponemes do not produce toxins or tissue destructive enzymes. Instead, disease is caused by autoimmune responses.
Treponema pallidum
Causes the STD syphilis. Transmitted by contact with open skin or vaginal, anal or oral sex.
- Stages of syphilis:
- Painless ulcer and painless regional swelling of lymph nodes.
- Rash on palms and soles. Condyloma latum, painless bumps on genitals. Almost any organ can be infected, resulting in fever, weight loss and lymphadenopathy (abnormal lymph node size).
- Most patients recover from the symptoms of the secondary stage, but 25% will relapse and develop the symptoms again.
- Slow inflammatory damage to organs, blood vessels and nerve cells. Patients either exhibit: Gummas (lesions of the skin and bone); Cardiovascular syphilis (aneurism of the aorta as the media layer becomes necrotic); Neurosyphilis (subacute syphilis, meningovascular syphilis where blood vessels of the brain is infected, tabes dorsalis damaging the spinal cord, general paresis leading to mental deterioration, or asymptomatic).
- Congenital syphilis:
- Early congenital - symptoms resemble adult secondary syphilis.
- Late congenital - similar to adult tertiary syphilis except heart damage is rare.
- Subspecies:
- Endemicum causes skin lesions that are mostly oral. Gummas of the skin and bone may develop.
- Pertenue causes the disease yaws. Papules and lesions appear on the skin, and later tertiary gummas develop in the skin and bones.
- Carateum causes the disease pinta. Papules develop, followed by lesions on the skin that turn blue in the sun.
Borrelia burgdorferi
Causes lyme disease, transmitted by insects.
- Stages of lyme disease:
- Early localized - a skin lesion at the site of tick bite, called erythema chronicum migrans (ECM). It is a rash that spreads out over time.
- Early disseminated - smaller, multiple ECM on the body. Four organs can be invaded:
- Brain and nerves: meningitis, cranial nerve palsies (especially Bell's palsy), and peripheral neuropathies.
- Heart: transient heart blocks and less commonly, myocarditis.
- Joint: brief attacks of arthritis.
- Late - chronic arthritis or chronic neurologic damage.
Borrelia recurrentis
Transmitted to humans by body lice. The bacteria spreads in the blood, causing a high fever, headaches and muscle aches. Symptoms relapse due to antigenic variation of surface proteins exhibited by the bacteria.
Leptospira
Transmitted to humans who come in contact with animal urine. In the first phase of disease: high spiking fever, headache and severe muscle aches, and red eyelids. In the second, immune phase: meningitis.
Leptospira interrogans can cause the more severe Weil's disease, or infectious jaundice. It causes renal failure, hepatitis, jaundice and hemorrhages in many organs.
Monday, February 3, 2014
Chlamydia and Rickettsia (Gram-Negative)
These bacteria are obligate intracellular parasites, meaning they can only survive inside animal cells. Chlamydia and rickettsia resemble viruses because of their size and parasitism. Unlike viruses, they can synthesize their own proteins, posses both RNA and DNA, and are sensitive to antibiotics. Chlamydia spreads from person to person, and rickettsia spreads from arthropod to person.
Chlamydia life cycle
The bacterium has a dense, small, inert form called the elementary body (EB). It is spread from cell to cell in the host, and becomes an initial body (IB), or reticulate body. IBs replicate before some are transformed back to EBs, which infect more cells.

Chlamydia trachomatis
Primarily infects the eyes and genitals, and causes STD.
Chlamydia psittaci
Infection is transferred from birds to humans. This bacteria common causes an atypical pneumonia called psittacosis.
Rickettsia rickettsii
Transmitted to humans by ticks. Bacteria proliferate in the blood vessel and capillary endothelium, and cause Rocky Mountain spotted fever. The skin rash of the disease is caused by small hemorrhages and inflammation.
Rickettsia akari
Transmitted to humans by mites. Causes rickettsialpox, which starts with a localized red bump on the bitten skin. The bump turns into a blister. Later, fever and headache develop and pox covers the body.
Rickettsia prowazekii
Causes epidemic typhus, especially in places of overcrowding, poverty and unsanitary conditions. (Epidemic is widespread and sudden. Endemic affects a population for a consistent time). Disease is transmitted by lice. Symptoms include fever, headache and small pustules on the skin. Unlike Rocky Mountain spotted fever, there is no rash on the palms, soles or face.
Rickettsia typhi
The endemic form of typhus, murine typhus, but symptoms are not as severe. Transmitted by fleas.
Rickettsia tsutsugamushi
Transmitted to humans by mite larvae. Causes scrub typhus.
Rickettsia parkeri
Infection started in the southeast coast of the US. Symptoms include fever, headache, eschar (scab) and regional lymphadenopathy (abnormal lymph node size).
Rickettsia africae
Causes African tick-bite fever (ATBF).
Chlamydia life cycle
The bacterium has a dense, small, inert form called the elementary body (EB). It is spread from cell to cell in the host, and becomes an initial body (IB), or reticulate body. IBs replicate before some are transformed back to EBs, which infect more cells.
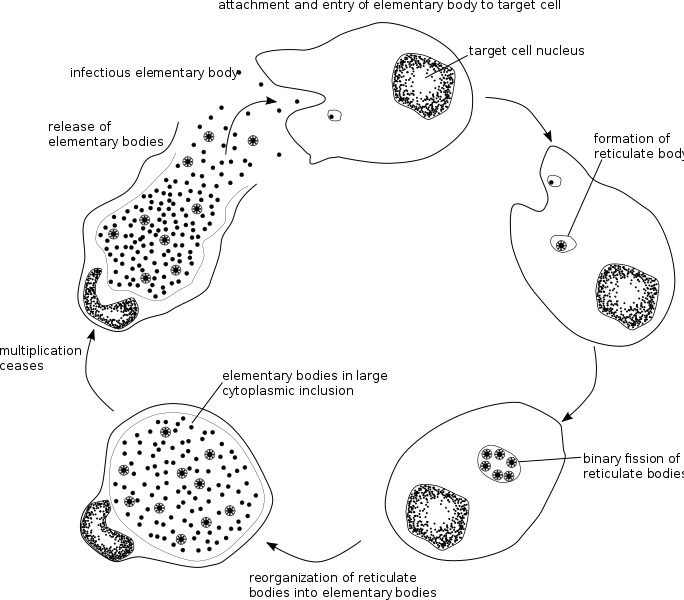
Chlamydia trachomatis
Primarily infects the eyes and genitals, and causes STD.
- Diseases:
- Trachoma, a type of chronic pink eye (conjunctivitis) and causes preventable blindness in the course of 10-15 years.
- Inclusion conjunctivitis of newborns by infection from the birth canal. Causes swelling, inflammation and pus.
- Infant pneumonia.
- Urethritis. As Neisseria gonorrhoeae most commonly causes urethritis, the disease caused by other bacteria is labeled nongonococcal urethritis (NGU).
- Cervicitis.
- Pelvic inflammatory disease (PID).
- Epididymitis, which can develop in men with urethritis.
- Lymphogranuloma venereum, an STD that exhibits painless bumps or ulceration on the genitals. Once bacteria migrate to the lymph nodes, the nodes swell and may break open.
Chlamydia psittaci
Infection is transferred from birds to humans. This bacteria common causes an atypical pneumonia called psittacosis.
Rickettsia rickettsii
Transmitted to humans by ticks. Bacteria proliferate in the blood vessel and capillary endothelium, and cause Rocky Mountain spotted fever. The skin rash of the disease is caused by small hemorrhages and inflammation.
Rickettsia akari
Transmitted to humans by mites. Causes rickettsialpox, which starts with a localized red bump on the bitten skin. The bump turns into a blister. Later, fever and headache develop and pox covers the body.
Rickettsia prowazekii
Causes epidemic typhus, especially in places of overcrowding, poverty and unsanitary conditions. (Epidemic is widespread and sudden. Endemic affects a population for a consistent time). Disease is transmitted by lice. Symptoms include fever, headache and small pustules on the skin. Unlike Rocky Mountain spotted fever, there is no rash on the palms, soles or face.
Rickettsia typhi
The endemic form of typhus, murine typhus, but symptoms are not as severe. Transmitted by fleas.
Rickettsia tsutsugamushi
Transmitted to humans by mite larvae. Causes scrub typhus.
Rickettsia parkeri
Infection started in the southeast coast of the US. Symptoms include fever, headache, eschar (scab) and regional lymphadenopathy (abnormal lymph node size).
Rickettsia africae
Causes African tick-bite fever (ATBF).
Friday, January 31, 2014
Yersinia, Francisella, Brucella and Pasteurella (Gram-Negative)
These are gram-negative rods that cause disease in animals, and are transferred from animals to humans. They are facultative intracellular organisms (with the exception of Pasteurella multocida), meaning the bacteria can survive within macrophages, set up infection to regional lymph
nodes of the site of contact, and infect organs via the bloodstream. Immune response is cell-mediated and exhibits delayed-type hypersensitivity.
Yersinia pestis
Causes bubonic plague. (Think rat and "pest"). This disease is still contractible in southwestern US.
Francisella tularensis
Causes tularemia, which closely resembles the bubonic plague. Infects many mammals, especially rabbits, and is carried by ticks and deerflies.
Brucella
Usually contracted from handling meat, and is common worldwide in countries where animals are not immunized or where milk is not pasteurized.
Pasteurella multocida
Not a facultative intracellular organism. Lives in the mouths of cats, and infects humans from cat or dog bite.
Yersinia pestis
Causes bubonic plague. (Think rat and "pest"). This disease is still contractible in southwestern US.
- Virulence factors:
- Fraction 1 (F1), antiphagocytic capsular antigen.
- V and W antigens, unknown function.
Francisella tularensis
Causes tularemia, which closely resembles the bubonic plague. Infects many mammals, especially rabbits, and is carried by ticks and deerflies.
- Diseases:
- Tularemia. Like the bubonic plague, symptoms include fever, swollen lymph nodes, and infection of multiple organs. Unlike the bubonic plague, there is no skin ulcer.
Brucella
Usually contracted from handling meat, and is common worldwide in countries where animals are not immunized or where milk is not pasteurized.
Pasteurella multocida
Not a facultative intracellular organism. Lives in the mouths of cats, and infects humans from cat or dog bite.
Thursday, January 30, 2014
Haemophilus, Bordetella and Legionella (Gram-Negative)
These bacteria infect the respiratory tract.
Haemophilus influenzae
Grows in the blood. Infects the lungs of patients who are weakened by the viral flu infection, and infects children who are at the stage of developing their immune system.
Haemophilus ducreyi
Causes the STD, chancroid.
Gardnerella vaginalis
Causes bacterial vaginitis with the presence of anaerobic vaginal bacteria.
Bordetella pertussis
Causes disease by toxin release, not bacteria-cell invasion.
Legionella pneumophila
Infection by airborne bacteria from contaminated water, but not person-to-person transmission. It survives phagocytosis and replicates intracellularly.
Haemophilus influenzae
Grows in the blood. Infects the lungs of patients who are weakened by the viral flu infection, and infects children who are at the stage of developing their immune system.
- Virulence factors:
- Polysaccharide capsule, of which there are six types: a, b, c, d, e and f. Capsule b is associated with the disease in children. Bacteria lacking a capsule can only cause local infection.
- Child diseases (type b):
- Meningitis (late-onset).
- Acute epiglottitis, swelling and inflammation of the epiglottis.
- Septic arthritis, where usually only one joint is infected from bacteria in the bloodstream.
Haemophilus ducreyi
Causes the STD, chancroid.
Gardnerella vaginalis
Causes bacterial vaginitis with the presence of anaerobic vaginal bacteria.
Bordetella pertussis
Causes disease by toxin release, not bacteria-cell invasion.
- Exotoxins:
- Pertussis toxin - like most exotoxins, its B subunit binds to the target cell receptors and gain entry. The A subunit activates G protein in target cell membrane and, in turn, activates intracellular messengers such as cAMP. In the case of pertussis, this signal causes:
- Histamine sensitization
- Increased insulin synthesis
- Increased lymphocyte production and inhibition of phagocytosis
- Extra cytoplasmic adenylate cyclase - this toxin is taken up by host neutrophils, lymphocytes and monocytes. Adenylate cyclase synthesizes cAMP, and in this case, weakens the defense cells' ability to lyse and phagocytose.
- Filamentous hemagglutinin (FHA) - pili that are responsible for attachment to bronchi epithelium.
- Tracheal cytotoxin - destroys ciliated epithelial cells, causing more buildup of mucus and bacteria.
- Diseases:
Legionella pneumophila
Infection by airborne bacteria from contaminated water, but not person-to-person transmission. It survives phagocytosis and replicates intracellularly.
- Diseases:
Wednesday, January 29, 2014
Hospital-acquired Gram-Negative Bacteria
Pseudomonas aeruginosa
The most problematic. Only infects weakened humans, and is very resistant.
Burkholderia cepacia
Transmitted to patients from water and drug resistant.
Stenotrophomonas maltophilia
Aerobic, part of normal respiratory flora, but can cause disease in immunocompromised patient.
Acinetobacter
Aerobic, causes a wide range of infections.
The most problematic. Only infects weakened humans, and is very resistant.
- Diseases (BEPSEUDO):
- Burn-wound infections.
- Endocarditis.
- Pneumonia by air contamination.
- Sepsis from infected catheters or from other sites of infection.
- External malignant otitis from an external ear canal infection.
- Urinary tract infection.
- (Diabetic) Osteomyelitis by wound infection, especially in diabetics who develop foot ulcers.
- Corneal infections in contact lens wearers.
Burkholderia cepacia
Transmitted to patients from water and drug resistant.
Stenotrophomonas maltophilia
Aerobic, part of normal respiratory flora, but can cause disease in immunocompromised patient.
Acinetobacter
Aerobic, causes a wide range of infections.
Tuesday, January 28, 2014
Enterics (Gram-Negative)
These are bacteria that live in the intestine, but can cause infection and disease. The enterics have varying but common cell surfaces: O antigen of the LPS, covered by K antigen capsule. H antigen, which is a subunit of the flagella, is present only in motile bacteria.
The main family groups are enterobacteriaceae, vibrionaceae, pseudomonadaceae and bacteroidaceae. Some groups contain many species, and are simply mentioned by their genus.
Pathogenesis
ENTEROBACTERIACEAE
Escheria coli
Constantly uptakes new DNA from conjugation, lysogenic conversion by bacteriophages and direct transposon mediated DNA insertion. If E. coli acquires virulence, it can cause disease, although it is part of normal flora in the intestine.
Klebsiella pneumoniae
Encapsulated (O) but non-motile (no H antigen). It is present in hospitals, causing sepsis and urinary tract infections via Foley catheters. Results in violent symptoms that can destroy lung tissues.
Proteus mirabilis
Very motile. See hospital-acquired infections.
Enterobacter
Very motile. Occasionally responsible for hospital-acquired infections.
Serratia
Can cause urinary tract infections, wound infections and pneumonia. Characterized by bright red pigment.
Shigella
This group has four non-motile species (dysenteriae, flexneri, boydii and sonnei) that are actually not part of normal intestinal flora, and are always pathogenic. Bacteria invade intestinal epithelial cells, and release the Shiga toxin, which disables cells' ability to reabsorb fluids and electrolytes. Diarrhea cause 2 (see Pathogenesis above).
Salmonella
Motile. Has Vi antigen capsule, similar to the K antigen, which surrounds the O antigen to protect it against antibody attack. Not part of normal intestinal flora, and always pathogenic. Lives in GI tracts of animals, and only infects humans when there is contamination of food or water with animal feces.
Yersinia enterocolitica
Not an enteric bacterium, but causes diarrhea (cause 3). Ingested from contaminated foods, such as milk for fecally contaminated water. Secretes exnterotoxin, similar to heat-stable senterotoxin of e coli. Fever, diarrhea, abdominal pain.
VIBRIONACEAE
Vibrio cholera
Causes cholera, a diarrheal disease (cause 1) from infection by fecal contamination. Multiplies in intestine, causing similar but more severe form of ETEC (see Escheria coli above). Toxin is called choleragen, with the same mechanism as LT toxin.
Vibrio parahaemolyticus
A marine bacterium that causes gastroenteritis after ingestion of uncooked seafood (sushi).
Campylobacter jejuni
One of the most common causes of diarrhea in the world, along with ETEC and rotavirus. Found in animals and infect humans by contamination of food or water.
Helicobacter pylori
Most common cause of duodenal ulcers and chronic gastritis (inflamed stomach) and second-most common cause of gastric ulcers.
BACTEROIDACEAE
Bacteroides fragilis
One of the few gram-negative bacterium that do not posses the endotoxin lipid A. This is a normally peaceful bacterium until it infects a wound and form an abscess. Fever and sometimes systemic spread accompany the infection.
Bacteroides melaninogenicus
Lives in mouth, vagina and intestine. Causes periodontal disease and aspiration pneumonia.
Fusobacterium
Causes the same diseases as B. melaninogenicus, abdominal and pelvic abscesses and middle ear infection.
The main family groups are enterobacteriaceae, vibrionaceae, pseudomonadaceae and bacteroidaceae. Some groups contain many species, and are simply mentioned by their genus.
Pathogenesis
- Causes of diarrhea:
- Release of exotoxins without entering cells of the GI tract. The intestinal epithelium reacts by losing electrolyte and fluid, causing watery diarrhea without symptoms.
- Invasion of intestinal epithelium destroys the cells by toxins and causes bleeding. Immune response causes fever.
- Invasion of the lymph and bloodstream causes abdominal pain, intestinal bleeding, fever and headache. A deeper invasion can cause lymph node enlargement, bacteremia and sepsis.
- Hospital-acquired infection - urinary tract infections, pneumonia, bacteremia and sepsis.
ENTEROBACTERIACEAE
Escheria coli
Constantly uptakes new DNA from conjugation, lysogenic conversion by bacteriophages and direct transposon mediated DNA insertion. If E. coli acquires virulence, it can cause disease, although it is part of normal flora in the intestine.
- Diseases:
- Diarrhea by strains:
- ETEC (Enterotoxigenic E. coli), cause 1 (see Pathogenesis above). Release of exotoxins heat labile toxin (LT) and heat stable toxin (ST) causes severe watery diarrhea, as by cholera.
- EHEC (Enterohemorrhagic E. coli), cause 1. Secretes powerful Shiga-like verotoxin. Blood in diarrhea.
- EIEC (Enteroinvasive E. coli), cause 2. Blood and pus in diarrhea, as by shigellosis.
- Urinary tract infection - acquisition of a pili virulence factor allows bacteria to travel up the urethra and infect the bladder (cystitis) and sometimes even the kidney (pyelonephritis).
- Neonatal meningitis.
- Gram-negative sepsis - usual and most common cause of hospital sepsis.
Klebsiella pneumoniae
Encapsulated (O) but non-motile (no H antigen). It is present in hospitals, causing sepsis and urinary tract infections via Foley catheters. Results in violent symptoms that can destroy lung tissues.
Proteus mirabilis
Very motile. See hospital-acquired infections.
Enterobacter
Very motile. Occasionally responsible for hospital-acquired infections.
Serratia
Can cause urinary tract infections, wound infections and pneumonia. Characterized by bright red pigment.
Shigella
This group has four non-motile species (dysenteriae, flexneri, boydii and sonnei) that are actually not part of normal intestinal flora, and are always pathogenic. Bacteria invade intestinal epithelial cells, and release the Shiga toxin, which disables cells' ability to reabsorb fluids and electrolytes. Diarrhea cause 2 (see Pathogenesis above).
Salmonella
Motile. Has Vi antigen capsule, similar to the K antigen, which surrounds the O antigen to protect it against antibody attack. Not part of normal intestinal flora, and always pathogenic. Lives in GI tracts of animals, and only infects humans when there is contamination of food or water with animal feces.
- Diseases (big 4):
- Typhoid fever.
- Carrier state - some people recovering from typhoid fever can become chronic carriers. They keep Salmonella typhi in their gallbladders, excrete the bacteria constantly and display no symptoms. Recall Typhoid Mary.
- Sepsis - bacteria in bloodstream carried to lungs, brain or bone. This is usually an infection of Salmonella choleraesuis and does not involve GI tract.
- Gastroenteritis (diarrhea) - most common symptom of this bacterium, caused by a cholera-like toxin that causes watery diarrhea (cause 1) with trace mucous and blood.
Yersinia enterocolitica
Not an enteric bacterium, but causes diarrhea (cause 3). Ingested from contaminated foods, such as milk for fecally contaminated water. Secretes exnterotoxin, similar to heat-stable senterotoxin of e coli. Fever, diarrhea, abdominal pain.
VIBRIONACEAE
Vibrio cholera
Causes cholera, a diarrheal disease (cause 1) from infection by fecal contamination. Multiplies in intestine, causing similar but more severe form of ETEC (see Escheria coli above). Toxin is called choleragen, with the same mechanism as LT toxin.
Vibrio parahaemolyticus
A marine bacterium that causes gastroenteritis after ingestion of uncooked seafood (sushi).
Campylobacter jejuni
One of the most common causes of diarrhea in the world, along with ETEC and rotavirus. Found in animals and infect humans by contamination of food or water.
Helicobacter pylori
Most common cause of duodenal ulcers and chronic gastritis (inflamed stomach) and second-most common cause of gastric ulcers.
BACTEROIDACEAE
Bacteroides fragilis
One of the few gram-negative bacterium that do not posses the endotoxin lipid A. This is a normally peaceful bacterium until it infects a wound and form an abscess. Fever and sometimes systemic spread accompany the infection.
Bacteroides melaninogenicus
Lives in mouth, vagina and intestine. Causes periodontal disease and aspiration pneumonia.
Fusobacterium
Causes the same diseases as B. melaninogenicus, abdominal and pelvic abscesses and middle ear infection.
Subscribe to:
Comments (Atom)